
Translate this page into:
Pulmonary parenchymal involvement by Classic Hodgkin Lymphoma – An unusual presentation
-
Received: ,
Accepted: ,
How to cite this article: Sarkar S, Mukherjee S, Kundu S, Chakrabarti S. Pulmonary parenchymal involvement by Classic Hodgkin Lymphoma – An unusual presentation. J Hematol Allied Sci 2022;2:18-20.
Abstract
Pulmonary involvement of Hodgkin’s disease is often encountered. However, presentation in the form of “pneumonia-like” consolidation is rare. A case is being described where a 31-year-old male patient presented with respiratory distress, intermittent fever, cough, and cervical lymphadenopathy for the past 2–3 months. Contrast-enhanced computed tomographic scan of thorax revealed a consolidation at anterior segment of the right upper lobe with atelectasis and mediastinal lymphadenopathy. CT-guided biopsy from the right lung lesion revealed infiltration by inflammatory cells mainly lymphocytes and eosinophils with presence of a few scattered atypical mononuclear and occasional binucleated cells. These atypical cells were immunopositive for CD 15 and CD 30 and negative for CD 45, CD 20, Epstein Barr Virus Latent Membrane Protein (EBV LMP 1), and multiple myeloma 1 (MUM 1). The final diagnosis was pulmonary involvement by Classic Hodgkin’s lymphoma. The present case is being depicted for its unusual clinical and radiological presentation.
Keywords
Pulmonary involvement
Consolidation
Histopathology
Immunohistochemistry
Classic Hodgkin lymphoma

INTRODUCTION
Pulmonary involvement occurs quite often during Hodgkin’s disease and accounts for almost 85% of the cases who present with the intrathoracic disease.[1] “Pneumonia-like” consolidation pattern is rare.[2-4] The current case pertains to an uncommon manifestation of pulmonary involvement by Hodgkin lymphoma.
CASE REPORT
A 31-year-old male patient presented with respiratory distress, intermittent fever, and cough for the past 2–3 months. Clinical examination revealed bilateral significant cervical lymphadenopathy. Chest radiography (PA view) showed pneumonia-like consolidation in the right lung [Figure 1a]. He was initially treated with antibiotics. However, his symptoms were not relieved. Thereafter, a contrast-enhanced computed tomographic (CECT) scan of thorax was done which revealed a consolidation at the anterior segment of the upper lobe of the right lung with atelectasis and mediastinal lymphadenopathy. The CECT scan of the lungs delineated the extent of the lesion. The lobular solid enhancing mass-like consolidation was encasing the right upper lateral mediastinal margin and right horizontal fissure. The right upper lobar bronchus with branches was seen to enter the mass and appear unobstructed as air bronchograms. Consolidation extended to RML with atelectasis of medial segment with air bronchograms [Figure 1b]. Subsequently, a CT- guided biopsy from the right lung lesion was undertaken. Histopathology delineated infiltration of lung parenchyma by inflammatory cells mainly lymphocytes and eosinophils with the presence of scattered atypical cells having convoluted bizarre nuclei and occasional binucleated cells having prominent nucleoli [Figure 2a]. These atypical and binucleated cells were immunopositive for CD 15 and CD 30 [Figure 2b and c] and negative for CD 45, CD 20, Epstein Barr Virus Latent Membrane Protein (EBV LMP 1), and multiple myeloma 1 (MUM 1). A diagnosis of “Pulmonary involvement by Classic Hodgkin Lymphoma” was rendered. Positron emission tomography (PET) CT was done, which revealed multiple hypermetabolic nodes, namely, bilateral cervical, and axillary, mediastinal lymph nodes besides the metabolically active large consolidation at the upper lobe of the right lung. The largest lymph node was in the right paratracheal region, measuring approximately 23 mm on short axis (Standardized Uptake Value [SUV] max 14.90).

- (a) Chest radiograph (PA view): Consolidation in the right lung. (b) CECT thorax: Mass-like consolidation at anterior segment of RUL with atelectatsis and mediastinal solid lymphadenopathy.
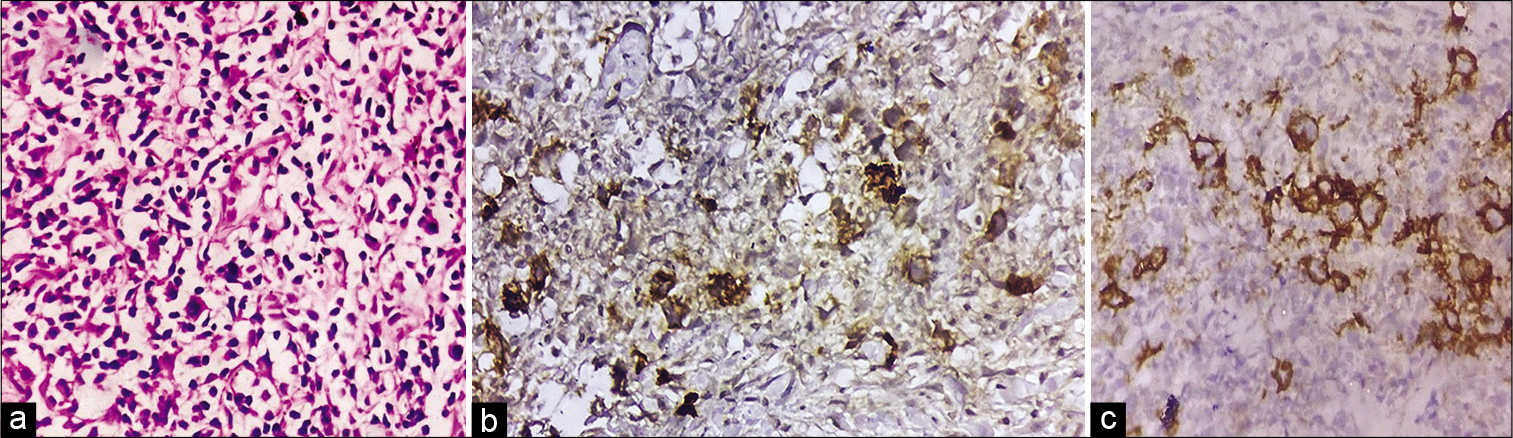
- (a) H&E, ×400: Infiltration of lung parenchyma by inflammatory cells predominantly lymphocytes, with few eosinophils and scattered atypical cells with bizarre convoluted nuclei, (b) Immunohistochemistry with CD 15 (DAB Chromogen, ×400): Atypical cells are immunopositive, (c) Immunohistochemistry with CD 30 (DAB Chromogen, ×400): Atypical cells are immunopositive.
The patient underwent left cervical lymph node excision biopsy, the histomorphology of which showed features of Classic Hodgkin lymphoma (CHL) and nodular sclerosis variant. Correlation of clinical presentation, radiological findings, histopathology and immunohistochemistry helped us to establish a diagnosis of secondary involvement of lung parenchyma by CHL. The patient was treated with six cycles of ABVD (doxorubicin, bleomycin, vinblastine, and dacarbazine) with complete resolution of the lesion on follow-up PET-CT.
DISCUSSION
CHL often involves the lung parenchyma during the disease. The pathogenic basis of the pulmonary involvement is believed to be secondary to lymphatic spread from regional lymph nodes or dissemination through the hematogenous route.[5] Lung involvement by CHL is characteristically in the form of multiple nodules or masses in radiology.[2] Presentation in the form of cavitary lesion or consolidation is relatively rare.
The mainstay for the diagnosis of CHL lies in the identification of RS cells and Hodgkin’s cells on tissue biopsy. Failure in considering CHL as a potential differential diagnosis poses a considerable lag in procuring tissue biopsy for an accurate diagnosis. Although Hodgkin’s disease commonly involves the mediastinum, secondary pulmonary parenchymal involvement is often encountered. Pulmonary involvement is encountered in 20% of cases at the outset of the disease, 40% during the clinical course, and 60% diagnosed at autopsy.[2] A study by Diederich et al. has delineated the CT findings of pulmonary involvement by lymphoma in 37 patients with recurrent or secondary Hodgkin’s disease and they found the most common CT findings to be nodules varying in size from 2 to 100 mm; while rare presentations comprised consolidation (27%) and direct extension from the mediastinum (27%).[2]
The current case presented with consolidation of the right upper lobe of lung, which was later diagnosed as lung involvement by Hodgkin lymphoma after an initial failed treatment with antibiotics. The remission rate of CHL following treatment is relatively high. Hence, lung involvement by Hodgkin lymphoma should always be a differential diagnosis in young patients who present with respiratory distress along with lymphadenopathy. The present case demonstrates an unusual pulmonary presentation of CHL in the form of consolidation in a young patient and thereby, emphasizes the importance of considering it in the differential diagnosis to ensure timely diagnosis and subsequent early initiation of therapy.
CONCLUSION
Pulmonary involvement by classic Hodkin Lymphoma (CHL) in a “pneumonia-like” consolidation is very uncommon. The present case raised considerable diagnostic dilemma because of unusual clinical and radiological features due to pulmonary involvement by CHL. Histopathological examination along with immunohistochemical study is essential for confirming lung involvement by CHL having unuasual clinical or radiological features.
Declaration of patient consent
Patient’s consent not required as the patient’s identity was not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Suidipta Chakrabarty is one of the Associate Editors of the Journal.
References
- The radiological spectrum of pulmonary lymphoproliferative disease. Br J Radiol. 2012;85:848-64.
- [CrossRef] [PubMed] [Google Scholar]
- Pulmonary manifestations of Hodgkin's disease: Radiographic and CT findings. Eur Radiol. 2001;11:2295-305.
- [CrossRef] [PubMed] [Google Scholar]
- Unusual radiologic and histologic manifestations of primary pulmonary lymphoma. Asian Cardiovasc Thorac Ann. 2014;22:362-4.
- [CrossRef] [PubMed] [Google Scholar]
- A 21-year-old male with productive cough, hemoptysis, chest pain, and weight loss. Respiration. 2007;74:706-9.
- [CrossRef] [PubMed] [Google Scholar]
- Hodgkin's lymphoma with unusual pulmonary presentations: Reporting two cases. Indian J Pathol Microbiol. 2017;60:272-4.
- [CrossRef] [PubMed] [Google Scholar]




